
Schizophrenia and schizoaffective disorder are two different disorders each with different diagnostic criteria and treatment though both are categorized as psychotic disorders. Both disorders include psychosis symptoms of hallucinations, disorganized thought process, and delusions though the differences include the presence of a mood disorder that is depression and/or mania as a diagnostic requirement of schizoaffective disorder, not for diagnosing schizophrenia.
What Is Schizophrenia?
It is a brain disorder that is chronic, with disorganized symptoms that can include disorganized speech trouble with thinking and lack of motivation. It can also display confusion, bizarre behavior, or abnormal movements. Cognition can be affected showing issues with concentration and memory and poor educational performance. Onset typically occurs in early adulthood. Men tend to show initial symptoms in their teens to early 20’s and women show initial symptoms often in their 20’s and early 30’s.
Characterized by disordered thinking (lasts at least 6 months).
Positive symptoms:
- Confusion about what is real or imaginary
- Preoccupation with religion
- Belief in clairvoyance
- Paranoia
- Delusions
- Hallucinations
- Heightened or dulled perceptions
- Odd thinking and speaking processes
- Racing thoughts or slowed down thoughts
Negative symptoms:
- Lack of friends
- Passivity
- Interacting in a mechanical way
- Flat emotions
- Decrease in facial expressions
- Monotone speech
- Lack of spontaneity
- Difficulty in abstract thinking
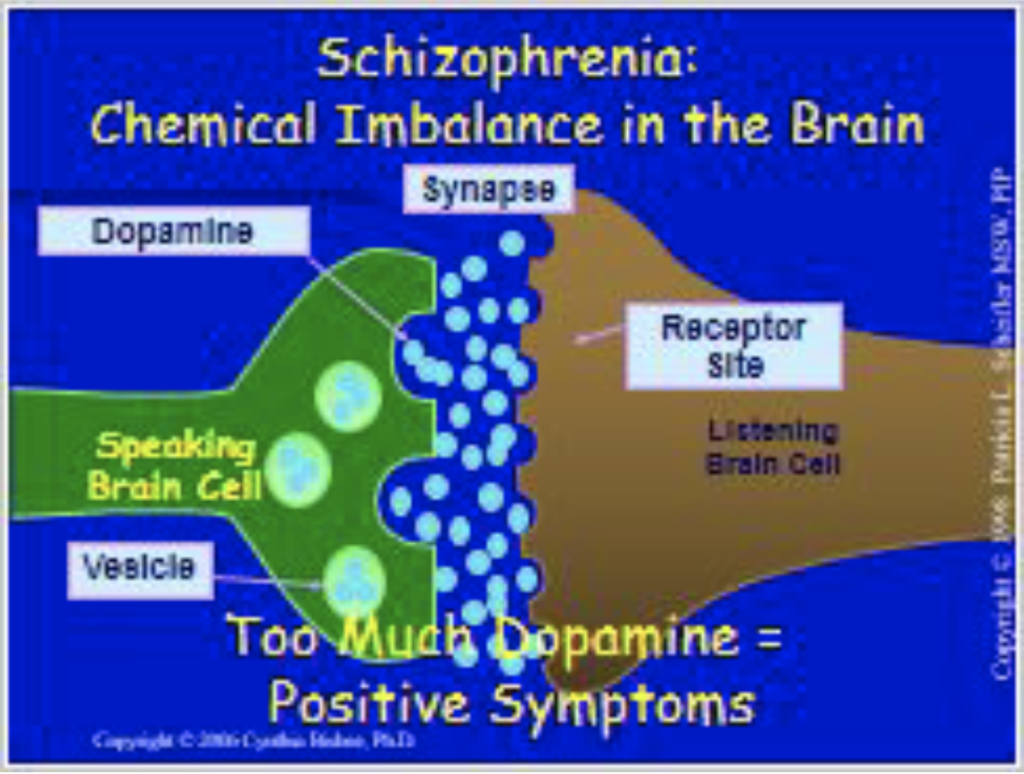
Research suggests there are links causing the onset of schizophrenia that may be stress induced events or biochemical abnormalities/chemical imbalances involving the neurotransmitter, dopamine. In a brain with schizophrenia the dopamine theory includes more transmitters are released between neurons causing the positive and negative symptoms.
What Is Schizoaffective Disorder?
Schizoaffective disorder is also a chronic mental health condition. There are similar psychotic symptoms displayed such as in schizophrenia: hallucinations, delusions, disorganized thinking, and flat affect, though there are also co-occurring symptoms of a mood disorder such as mania and/or depression.
An individual diagnosed with schizoaffective disorder will be diagnosed with either bipolar type or depressive type. Symptoms of mania are characterized as excess in behavioral activity and can include euphoria, expansive mood, irritability, inflated self-esteem, or grandiosity, decreased need for sleep, talkativeness, racing thoughts, distractibility, increased goal directed activity, and/or excessive involvement in pleasurable activities with high potential for negative consequences.
Symptoms of depression include depressed mood most of the time, diminished interest, or pleasure, change in appetite and/or weight, change in sleep pattern, change in activity level, fatigue or loss of energy, feelings of worthlessness, hopelessness, and helplessness, inappropriate guilt, recurrent thoughts about death, decreased concentration or ability to make decisions.
Primary diagnosing criteria:
- Rule out other medical conditions
- Rule out substance abuse
- A duration in which a major mood disorder [mania, depression] occurs at the same time as psychosis symptoms are present [hallucinations, delusions, disorganized thoughts]
- Psychosis symptoms for two or more weeks in the absence of a major mood episode.
- Symptoms for the mood episode meet diagnostic criteria and are present for most of the illness.
Positive symptoms:
- Hallucinations
- Delusions
- Thought disturbances
Negative symptoms:
- Blunted affect
- Apathy
- Anhedonia
- Poverty of speech or content of speech
- Inattention
Prevalence and Statistics
Schizophrenia affects less than one percent of the U.S. population. Schizoaffective disorder affects 0.3 percent of the U.S. population. The onset of schizophrenia and schizoaffective disorder begins in both men and women in their early 20’s, however men may experience symptoms as early as their teens and women as late as their 30’s. Both disorders include psychosis symptoms of hallucinations, delusions, disorganized thinking, and flat affect while schizoaffective disorder must have an accompanying mood disorder.
For schizophrenia symptoms are chronic and persistent; schizoaffective disorder’s psychotic symptoms come in episodes.
Risk Factors
Untreated schizoaffective disorder and schizophrenia may lead to impared functioning in the domains of occupation, socialization, education, housing, and family. In some cases, it may also lead to self-harm, suicidal ideations, or homicidal ideations, and paranoia.
Treatment and Coping
Schizoaffective disorder and Schizophrenia are treated and managed in several ways:
- Medications, including mood stabilizers, antipsychotic medications, and antidepressants
- Individual, group, and family psychotherapy such as cognitive behavioral therapy or family-focused therapy
- Self-management strategies and education
- Life skills training for social and vocational skills
- In some cases, inpatient hospitalization is necessary to stabilize symptoms
- For continued stabilization and skill streaming, residential mental health treatment is recommended.
Coping Skills
- Learn about the disorder
- Pay attention to warning signs
- Join a support group
- Avoid recreational drugs, tobacco, and alcohol as these can worsen symptoms and interfere with psychotropic medications.


